
RCGP Council review 21.2.20
RCGP Council meeting review 21.2.20
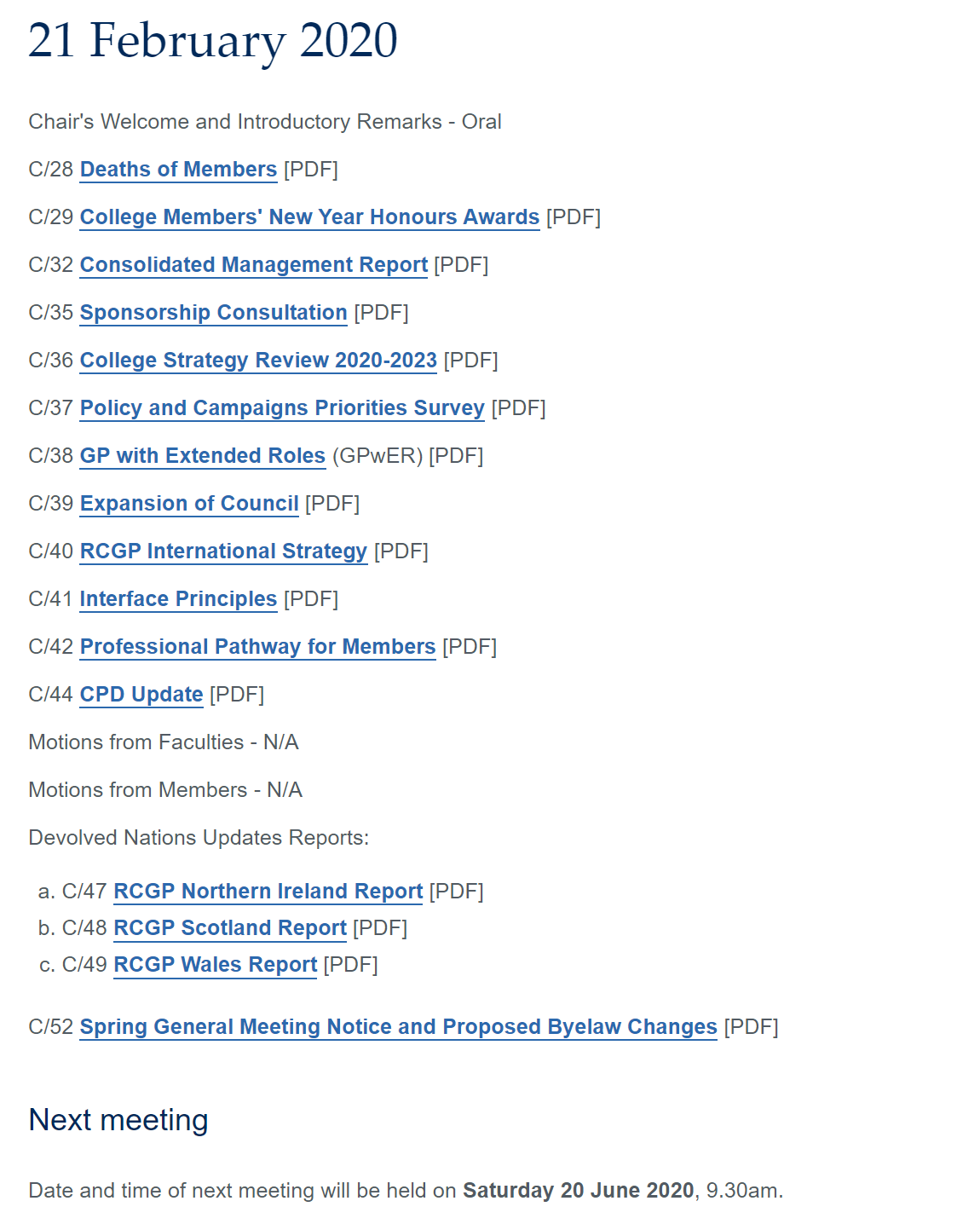
RCGP Members can access minutes here: https://www.rcgp.org.uk/council-papers.aspx
Welcome and Chair report by Martin Marshall.
Approval of standing orders and apologies for absences, DOI and IG and welcome of first-time faculty reps, other seats, and observers.
Chair general announcements
Martin Marshall commented on recent issues including coronavirus and the challenges it proposes. Also, the GDPR element of the RCGP Council was raised. I feel this was directed at my own efforts where I shared an audio recording of my own words relating to the Romeny report. I confirm I only shared my words but I am aware the college feels this should be cautioned relating to recordings (see my last report).
I maintain that for transparency, the RCGP council should be open to members and recordings of my own words are not a GDPR issue as I have given my consent. I hope the college progresses with its aims for transparency to the point that the council is live-streamed in the near future.
On a positive note, we acknowledged the honours awarded to Dr Jonathan Leach and Dr Victoria Tzortziou-Brown
Review of trustee board minutes –
Various issues were discussed. Notable was the budget of the RCGP which with the changing nature of our membership needs to shift to a cost-neutral basis after a few years of investing more in college resources.
Of note, was comments about the fact AiTs have no choice but to be members (not completely true but it is inhibited) and more accurate data showing membership balance would be more effective. This created an interesting discussion
Additionally, Dr Margaret McCartney was officially voted in as a member of the RCGP board of trustees. Congratulations Margaret and I welcome the additional rigor and challenge you will bring to our college’s decision body.
Papers for decision
Assisted dying debate.
The highest responded consultation in the history of the college. The results as follows:
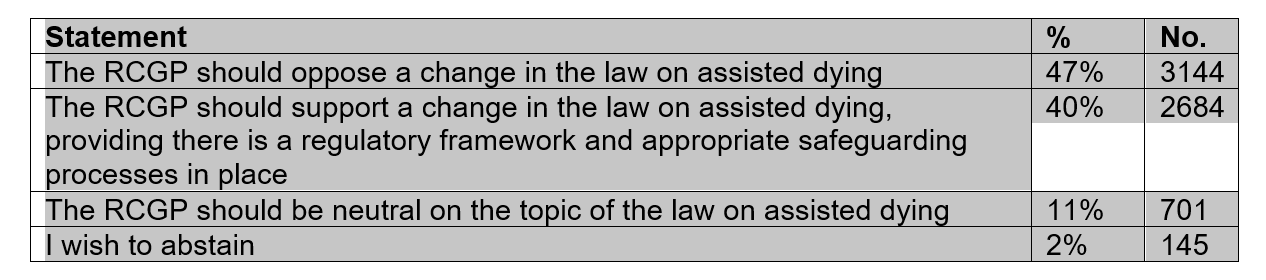
Interesting points made that although the majority is not to change the college position, that in fact, the cumulative votes show a change either to opposition or neutrality. This was also challenged from an academic perspective.
Also, some comments were made about the process and engagement including a question on whether the option to vote was available to all members given comments to some members stating they did not get the email.
A reminder that the consultation was to find opinions, not a vote. Key comments were made about the timeframe of the vote being brought back to the council before a five year period.
Votes were held (apologies the wording may not be exact but the themes are true).
The RCGP will continue to hold the view to oppose a change in the law on assisted dying. I voted no.
Yes 44
No 13
Abstain 5
The Council will not review this decision for 5 years unless a significant change is suggested otherwise. I voted yes.
Yes 55
No 6
Abstain 1
Break
Sponsorship consultation
This paper was brought forward to discuss noting the final decision will be made by the trustees of RCGP Council due to the financial implications, particularly on the RCGP conference and costs of the RCGP college.
The view was that the document was thorough and explained the issues clearly and much better than previous consultations.
Multiple views were discussed including clarification of different areas and the complexity they hold ie, charities may be acceptable, but what if they are drug sponsored, pharma may be opposed but not medical technology companies who can be considered the same, and exclusions such as newer biotech companies and internet providers.
Two votes were held
‘Approves the principle of transparency to be added to the other five principles of the sponsorship policy. In particular, agrees that “A list of all College sponsors (other than donations) should be published annually on the College’s website with information on the bandwidth of amounts of sponsorship (e.g. <£5 K, £5-10 K etc.)”
Yes 60
No 1
Abstain 0
Decides on whether any of the following needs to be added as a “red line” in the policy:
- · Cosmetic surgery providers
- · Private Healthcare providers
- · Pharmaceutical Industry
- · Non-prescribed, non-evidence based (e.g. not approved by SIGN/ NICE) nutritional products and foods
1 – 28 votes
2 – 8 votes
3 – 11 votes
4 – 35
Non – 19
RCGPs 2020-2023 college strategy
This paper was received as below
The paper confirmed the following priorities:
· Deliver practical solutions to tackle workload pressures and sustain and equip GPs to provide the best possible patient care.
· Develop the College into a dynamic and inclusive membership community.
· Promote the contribution of general practice and the role of the GP.
· Ensure members place a high value on their College membership.
Initially, little debate seemed to develop but this snowballed with comments about priorities for members vs others with the growing diversification of the primary care workforce and how supervision will impact GPs. Also taking note of other roles in General Practice particularly noting private providers.
RCGP campaign priorities
Key points are based on a change to three-year priorities to promote effective working. The priorities for the next three years are:
– Reducing unnecessary general practice workload
– Sustainable infrastructure for general practice
UK Council Chair Martin Marshall’s Priority is:
– Reinvigorating relationship-based care
GP with extended roles
An interesting debate on the pro and cons of formalising GPs with extended roles. On how it can lead to more certificateitis (like smears and Spirometry) and limitations but also offers protection to those clinicians working in more challenging areas like rural medicine (like BASICS).
The hope from the document is that it highlights the specialist generalist idea and would continue as it stands.
Professional Behaviours and Communication Principles for working across Primary and Secondary Care Interfaces in Northern Ireland
This paper looks at the ‘By Choice- not chance’ document and based on the ‘#DearColleague’ effort to talk with respect and equality between GPs and secondary care and the quality of communication between primary and secondary care.
This excellent document showcases 10 points listed below
1) Leading by example, always be respectful of colleagues in front of patients or other colleagues. Be particularly mindful of your attitudes and the language you use in front of medical students and trainees – your behaviors can have a considerable impact on how they view and value the various professions.
2) Everyone should have active consideration of the workload and pressures facing other colleagues. All clinicians’ workloads will involve issues about which you may not have any understanding or concept.
3) If a doctor is aware of significant changes in treatment or there is an important or unexpected change in the status of the patient, it is important to update all who need to know quickly. Minor amendments can be communicated through the usual methods.
4) When transferring a patient to the care of another colleague (or seeking an opinion) ensure that all the information that colleagues may need is sent to them in a clear and concise format, ideally outlining a specific aim where appropriate.
5) Be mindful of your communication with patients – give them all the information you can, using appropriate language and avoiding unreasonable expectations. A lack of clear information can cause issues when they see their next healthcare professional. The Academy of Medical Royal Colleges has recently provided relevant guidance on patient communication.
6) Try not to commit other individuals or teams to any particular action or timescale without checking that it is reasonable and practicable.
7) Try not to hand over work to a colleague in another team if you or a member of your team can do it, unless you are sure that the task can be done more appropriately elsewhere. When handing over care, check that all relevant tests and treatment plans have been instigated, where practicable, and plans are in place to forward additional information, when available.
8) Remember it is the responsibility of the requesting doctor, and/or their clinical team, to review the results of any test requests and take appropriate action.
9) If one colleague is unsure whether another can take responsibility (e.g. for ongoing care, prescribing or monitoring), get in touch directly and confirm the course of action.
10) If contacted by a professional colleague, make every effort to respond to them as quickly as possible or pass them onto another individual who can respond.
This work is exemplified by the RCGP Vale of Trent faculty in their video about the primary and secondary care interface and similar scheme getting GPs and secondary care clinicians in the same room.
A great suggestion to adapt the process of joint GP and consultant teaching where a topic is taught by both a GP AND a specialist at the same time.
Professional Development Pathways: Introducing the concept
This was a welcome paper that does need renaming as pathways is seen as not the right name. It was recognised that the RCGP can do this work and well if pitched correctly and should encourage the portfolio working of our peers.
A key request for developing the networks to support the learning was made.
Tackling the Climate Crisis: How we can make a difference’. The RCGP Climate Emergency Task & Finish (T&F) virtual Group’s interim report
This paper was received for noting. It was not without controversy as the authors of the papers have contacted council members directly to request alternate recommendations are adapted. This was felt to be a grievous breach of process and impact the tone of discussion. However, it was recognised what can be done in contrast with the membership voting to not have the climate crisis as a key priority for the college.
A costed report will be brought to the June council meeting.
CPD update
Was received with a clear focus on digital aims and integration for member benefit.
No other papers were discussed next meeting Sat 20th June.